





April 10, 2014
Posted by Brooker in
Isoinertial Training Concepts
This is the first publication I have created for elite-training.ch and it is a shortened version of an academic essay titled 'Isoinertial Training Concepts' comprised for my MSc. I will typically be posting modifications of university essays (in english, german readers might google translate it) and posting these online if they contain sufficient content, however if there is something of particular interest that someone would like to read then please contact me; brooker@elite-training.chNote: We have no affiliation with Desmotec and receive no compensation for this article.
Introduction
In the 1980’s a doctoral student named Hans Berg from Karolinska Institutet (Stockholm, Sweden) pitched an idea to his mentor, Per Tesch, a solution to strength training in a microgravity environment. He explained the basic idea of a gravity-independent ergometer; using a simple yet special setup, a flywheel (FW) axle fixed to a frame, with a strap winded onto its shaft and the other end connected to a harness, handle or leg pads. The trainee would pull the strap for its entire length during a concentric muscle action and thus setting the flywheel into motion. At the end of this motion, the flywheel continues to spin due to its inertia and recoils the strap with which the trainee resists and decelerates the flywheel until its kinetic energy is dissipated and comes to a halt. During the resistance (eccentric) phase the movement is exerted over a smaller angular displacement compared to the concentric phase, creating a higher torque during the recoil and therefore creating eccentric overload.Here at G.E.T we recently purchased a flywheel device after reading interesting scientific publications and hearing rave reviews from Scandanavian and Swiss national ski teams. Desmotec TM Technology commercializes a training instrument named ‘D-11’ which was originally designed to focus on eccentric overload of the quadriceps and adductors as well as supporting trunk musculature whilst unloading the shoulder complex and spine. The product comes with shoulder harness, hip belt and double handle with which many exercises can be performed with altering variations.
The resistance of a flywheel is nearly unlimited and self-adjusting, since the flywheels inertia opposes the force exerted. This suggests that all repetitions are performed maximally (especially without experienced use) which can pose positives and negatives depending on perspective and context of use. The athlete can train using the isoinertial device until exhaustion; despite force production decreases with fatigue and the flywheel can easily accommodate variations in force over an entire range of motion. This can be helpful since different joint angles can be trained and analyzed, athletes with altering biomechanical efficiency can still use the device with simple modifications.
The D-11 can test; power curve, test of power (single set of 10 repetitions at maximum exerted force), control test, test of balance, isometric test. For the last three tests mentioned, the inclusion of force plates are needed and the D-11 has enough ports for four force plates to be attached. The software offers real time; peak power values for both concentric and eccentric action displayed as repetitions or over continuous series. The system automatically counts sets, reps, recovery time, execution time and discs used. Users can also create a profile for individuals or teams, where all recordings are stored and a report can be printed at any time.
Much research has been conducted on the benefits of eccentric overload training in raising neural and muscular performance and in the rehabilitation and prevention of injuries. Some benefits include; higher forces are generated compared with traditional concentric action (LaStoya et al., 2003), unique neuromuscular activation which can be trained specifically (Enoka, 1996), stimulate specific micro-adaptations to regenerate a stronger muscle tissue (Brandenburg and Docherty. 2002), lower pulmonary stress compared to other forms of training (Abbott and Bigland. 1953), effective in injury rehabilitation (LaStoya et al., 2003; Lorenz and Reiman. 2011), increased hypertrophy adaptations when compared to other forms of training (Brandenburg and Docherty., 2002).
Injury Rehabilitation
Unaccustomed eccentric activity frequently results in muscle damage, which is expressed as pain, tenderness and strength loss (Howell et al. 1993). It is generally accepted that muscle injuries typically occur when a muscle under tension is overstretched beyond its limits, and Garrett (1990) has shown that high velocity eccentric action causes greater muscular damage than slow velocity (however this study looked at only untrained subjects). With the increased level of muscle soreness experienced with eccentric overload this would typically pose a problem implementing it into a training plan, however Nosaka et al. (2001) demonstrated the ‘repeated bout effect’. After full recovery has been achieved following the first eccentric overload bout, a repeated training results in minimal symptoms of muscle damage allowing eccentric overload to become a viable training means, especially when considered that the ‘repeated bout effect’ can last for several months (Nosaka et al. 2001). The exact mechanisms are not well defined but it seems to involve neural, mechanical and cellular adaptations (Nosaka et al. 2001).Arguably one of the most effective techniques for muscular, tendon and ligament rehabilitation is the use of an eccentric focused protocol (Lorenz and Reiman, 2011). The effectiveness of eccentric training in rehabilitation is not new, Bigland and Woods (1976) found: less muscle activity is required to maintain the same force during eccentric action, less muscle fibers are needed to exert a specific force value and also a significant reduction in oxygen uptake during lengthening. Previous work made by Abbot and Bigland (1952) supports this theory and since then it has been common knowledge that eccentric execution results in greater force production with less energy expenditure and less oxygen consumption compared to concentric execution. Recently extensive research has confirmed the effectiveness of eccentric training in the rehabilitation of hamstring muscle strains, tendinopathy and anterior cruciate ligament (ACL) rehabilitation (Lorenz and Reiman, 2011)
The efficiency of using eccentric overload on a flywheel device has been conducted on healthy, elite sporting level subjects (Askling et al. 2003, Tous-Fajardo et al. 2006), injured highly trained athletes (Romero-Rodriguez et al. 2011) and recovering knee injury patients (Greenwood et al. 2007).
Greenwood et al. (2007) commented that the use of a non-gravity independent ergometer is as safe and as effective as standard training equipment for ACL deficient and ACL reconstruction patients. From the results it appears that the flywheel (FW) does offer superior eccentric resistance when compared to a traditional weight stack machine (WS), however this difference is not very big. It is discussed of the possibility of superior effects from the FW with a longer training period, since significant improvement from mid-test to post-test which may indicate performance was improving when the training was terminated. This makes logical sense as full ligament recovery typically takes longer than the study was performed.
Hamstring injuries are considered one of the most common and frustrating soft tissue injuries in elite athletes. An interesting study done by Askling et al. (2003) split 30 elite soccer players into two groups to examine the effectiveness of eccentric overload using an insoinertial leg curl device. The mechanism of hamstring injury is typically during the terminal swing phase during sprinting, just prior to foot contact, where the hamstrings are near maximal length and are eccentrically contracting to decelerate the leg and prepare for contact (Schache, 2009). At this ‘moment' there is a rapid, forceful contraction that is elongated over two joints with minimal sarcomere overlap (Jonhagen et al., 1996). One group of players performed 16 sessions of specific hamstring training (4 sets of 8 repetitions) using the flywheel leg-curl during preseason, with the control group performing no specific hamstring exercise. The training group clearly had a lower occurrence of hamstring injuries (3/15) compared to the control group (10/15) at the end of the season. It is also worth mentioning that there were significant (p<0.05) increases in strength (isokinetic concentric and eccentric muscle strength) and speed (30m sprint) shown in Table 1. A possible explanation for the reduction in injury occurrence may be explained via EMG results; higher ratio of ecc/conc of biceps femoris (BF) compared to semitendinosus (ST). Tous-Fajardo et al. (2006) proposes that BF plays the most critical role of decelerating compared to ST and BF is the most commonly injured muscle in the hamstrings complex. The flywheel appears to train this particular ‘window’ (30o knee flexion) much more effective than typical weight stack leg curl machines (Tous-Fajardo et al., 2006).
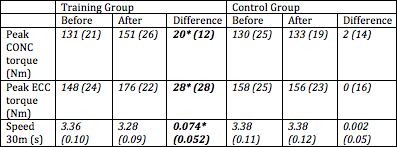
Table 1 Mean values and SD in training and control groups for concentric (CONC) and eccentric (ECC) strength. peak torque and 30m sprint. *denotes significant difference p<0.05. Askling et al. (2003)
Romero-Rodriguez et al. (2011) examined the efficacy of a short-term, low-frequency (<24 minute contractile activity, 12 exercise sessions over 6 weeks) isoinertial eccentric overload programme in the reduction of pain from long-term (>30 weeks) patellar tendinopathy. A distinct clinical improvement was reported as well as increased strength and neuromuscular activation. There was an overall robust increase in muscular strength with significant increase in eccentric force and no significant concentric mean force improvement. This may be due to the exercise design, trainees were told to produce maximal force in CONC action, modest ECC action at beginning and focus on the last third of the ECC movement – whereby ECC overload is produced. At first this may seem impractical with less force and more tendon strain, however it seems that this can be tolerated and reduce pain and symptoms of patellar tendinopathy (Jonsson and Alfredson, 2005). After post-test MVC, a correlation between increase in rectus femoris (RF) activity and eccentric strength was discovered. With such a small subject group (n=10) and extra sports activities not restricted it is hard to make this conclusive. Another factor to take into consideration is inter-individual variation in subjective pain and muscle strength in MVC.
Hypertrophy
Much research has outlined the increased contractile properties and muscular hypertrophy in humans from eccentric training. Moore et al., (2005) found a rapid rise in myofibrillar protein synthesis after maximal eccentric actions compared with maximal concentric. When looking at the results from isoinertial training compared to standard concentric/eccentric actions, the following adaptations have been outlined with greater; protein synthesis, cellular signaling for protein synthesis, myofibril disruption, Z-Line streaming and ultrastructural changes (Norrbrand, 2008). In the process of muscular hypertrophy, eccentric loading is crucial (Brandenburg and Docherty. 2002), so optimizing the stimuli with eccentric overload from the use of the FW device seems logical (Norrbrand, 2008). This is supported with work from Brandenburg and Docherty (2002) who show eccentric training attenuates a greater rate of hypertrophy than concentric training.Cellular signaling and increased protein synthesis may occur after a single bout of resistance exercise (Chesley et al., 1992). However, it is typically agreed that neural adaptations are the first response to resistance training programmes and following muscle hypertrophy is evident after some weeks, which progressively aids to improved strength and performance (Norrbrand, 2008).
Norrbrand et al. (2008) studied two groups of men with comparable physical characteristics and training history. Seven men were assigned to perform the resistance training protocol (left limb CONC-ECC knee extension) with a FW device and 8 men utilizing an identical protocol but with a weight stack machine. 4 sets of 7 reps were performed two and three times weekly with individualized weights to result in failure to lift and control the eccentric portion. A turning point was used for the WS group to control range of motion, which would match the FW angles. Figure 1 shows left quadriceps muscle volume increased by 6.2% (p<0.025) in the FW group compared to 3% increase for WS (p<0.025).

Fig. 1 Relative change of muscle volume in individual quadriceps muscles following training procedure from flywheel training (upper graph) and weight stack (bottom graph). * denotes significant (p<0.025) increase from pre to post. § denotes trend to different response for VL in WS compared with FW (p<0.10). Graph taken from Norrbrand (2008)
Another very similar unilateral study showed a near identical result. Tesch et al. 2004 had 10 middle aged men and women perform 4 sets of 7 maximal repetitions two or three times per week for 5 weeks. MVC and electromyography (EMG) activity of vastus lateralis (VL), vastus medialis (VM) and rectus femoris (RF) were measured before and after the intervention with magnetical resonance imaging (MRI) assessed throughout the protocol. Table 2 displays analogous to Norrbrand et al. (2008), quadriceps muscle volume increased by 6.1% (p<0.05).
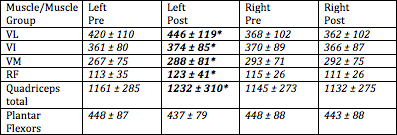
Table 2 Volume (mL) of individual quadriceps muscles and muscle groups pre and post FW training regime. Left is trained limb, right is untrained. Values are mean ± SD. * denotes differences between pre and post p<0.05. Tesch et al. 2004.
Strength and Neural Adaptations
Due to neural adaptations, neuromuscular efficiency, reduced inhibition and increased recruitment of high threshold motor units maximal strength increases are generally greater than muscle hypertrophy response following a strength training programme (Norrbrand, 2008). Since a trainee can lower 40-50% more weight than they can concentrically lift, there is a big limitation in traditional weight training programmes thereby not optimizing on the specific eccentric induced adaptations.Norrbrand (2008) proposes an advanced neural adaptation augmented from chronic eccentric overload training, since results show training dynamic and isometric strength leads to more eccentric overload when compared to pure concentric actions or coupled concentric-eccentric actions.
Norrbrand et al. (2011) set out to examine the adaptation difference between the ‘gold standard’ lower body strength exercise; barbell squat (BS) and a FW device. They had 5 resistance-trained subjects perform three MVCs followed by 5 sets of 10 maximal repetitions of squat exercise; utilizing either a FW device or traditional barbell on separate days. Using functional MRI scans; quadriceps muscle use was assessed before and within 3 minutes after finishing exercise. The exercising VM, VL and RF were tested for force and linear displacement during the exercise. The FW provided greater peak force during ECC and CONC (p<0.05) than compared with BS. Transverse relaxation time (T2) was increased more with the FW device than with BS (Fig.2) highlighting a unique adaptation. Furthermore it was found that T2 increased in RF greater than vastii (p=0.037), which was not found in BS. EMG results found normalized EMG root mean squared (RMS) of VM, VL and RF was greater with FS than BS (p<0.05) demonstrated in Figure 3.
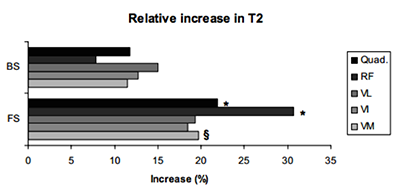
Fig.2 Relative T2 change in quadriceps total and individual quadriceps muscles from barbell squat (BS) or flywheel (FS). *denotes greater T2 increase in FS compared to BS (p<0.05). § denotes greater T2 increase trend. Taken from Norrbrand (2008)
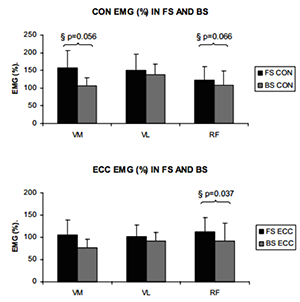
Fig.3 Normalized EMG activity in vastus medialis, vastus lateralis and rectus femoris in CONC and ECC actions during FS and BS. § denotes trend to greater normalized EMG activity in FS compared to BS. Taken from Norrbrand (2008)
To explain the interesting results in muscular hypertrophy previously reported by (Norrbrand et al. 2008; Tesch et al. 2004) Pozzo et al. (2006) set out to compare neural adaptations in untrained subjects following a resistance training programme using either a FW device or WS. It became evident that near maximal activation was present in major portions of CONC and ECC actions in the FW group when compared to the WS. FW elicited maximal EMG throughout a major part of the CONC action and maximal/near maximal in the flexed position of ECC action due to the FW’s inertia. EMGconc was very similar between the two groups however EMGecc was much higher in FW, thus appearing to be more of an optimal stimulus for hypertrophy. MVC increased by (p<0.05) 8.1% for the FW group compared to 4.8% in WS. Maximal EMGrms of VL increased (p<0.05) in FW but not in WS. The maximal EMGrms of VL from FW resistance may indicate increased neural drive, but uniquely to FW the MVC results appear to correlate with associated hypertrophy reported elsewhere, which contradicts neural drive. A near identical repeat of this study should be completed since the study design was robust to gain further knowledge in this area.
The combination of increased strength and musculature hypertrophy was also found in the previously mentioned Tesch et al. (2004) study, whereby they reported an 11% increase in average CONC and ECC force generated during exercise (p<0.05). This appears to have led to an improvement (p<0.05) in MVC (90o and 120o) of 11% and 12% respective in post testing.
The neurological benefits of isoinertial training appear from all of the studies found. Norrbrand et al., (2011) demonstrated ECC peak force exceeded (p<0.05) CONC peak force pre and post training with FW device, inferring eccentric overload is possible from the first session. Norrbrand et al., (2011) also found increases in MVC at 90o from FW training at an 11.6% increase. No interaction was found across limbs and time in MVC at 90o WS group (Fig.4).
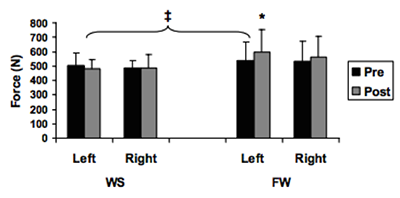
Fig. 4 Maximal isometric force (MVC) at 90o of left (trained) and right (untrained) limb pre and post training in FW and WS groups. * denotes increase from pre to post (p<0.025). ± denotes different response for left limb across groups (p<0.05). Graph taken from Norrbrand (2008)
A study utilizing the Desmotec D-11 was performed by Baricich et al. (2013) whereby a development with FW training was discovered. They exhibited greater peak force with increased inertia. The ECC peak force was greater than CONC in experienced subjects and average ECC force increased with increased moment inertia. Peak velocity was higher during ECC than CONC regardless of inertia highlighting isoinertials unique ability to create eccentric overload. This is also supported by Tous-Fajardo et al., (2006)
An interesting study designed by Onambele et al. (2008) had 12 subjects increase knee extensor peak isokinetic power by 28% (p<0.01) with a FW device with no change in weight lifting group. They discovered a transfer/overspill of the physiological adaptations with gastrocnemius stiffness increasing by 136% in FW compared to 54% for WL (p<0.01), this improvement was correlated with an improvement in postural balance (p<0.01). This study looked at improvements in strength and postural balance in older individuals (69.9+/-1.3 years), however the sports performance benefits of increased tendon stiffness warrants more research to be done in this area as well as further research into isoinertial training itself.
Conclusion
The use of a FW device and therefore performing isoinertial training has showed an increased level of; muscular hypertrophy, strength, speed, rehabilitation and prehabilitation. EMG results show no increase in muscle spine activity (Baricich et al. 2013) suggesting the FW could potentially be a valuable tool in resistance training and in rehabilitation settings. Since eccentric overload can be attained in the first session, delayed onset of muscle soreness diminishes fast, the repeated bout effect can last for many months and once experienced the physiological benefits occur with less effort it appears an efficient technique to promote the aforementioned biological adaptations. However, it is certainly not the holy grail, more large scale robust studies are required, but it may be a useful tool in an athlete's GPP (general physical preparation), rehabilitation, or SPE (specialized preparatory exercise) for skiers and snowboarders.If anybody has some experience, comments or questions please post below
-Brooker



 74%
74%Schreib einen Kommentar
© 2018 - Elite Training GmbH
